Adolescent Idiopathic Scoliosis
What is it?
Scoliosis is a lateral curvature of the spine (> 10°) in the frontal plane with accompanying rotation of the vertebrae about a longitudinal axis. More specifically, adolescent idiopathic scoliosis (AIS) is a scoliosis of unknown origin that affects children between the ages of approximately 10 and 18 years of age.
Who gets it?
AIS affects approximately 2 percent of children between the ages of 10 and 16. AIS of small curvatures occurs with equal rates in both boys and girls in that age group. However, curves of larger magnitudes (> 30°) occur ten times more often in females then in males. Females also have a greater risk of progression. The prevalence of curves greater than 30° is 0.2 percent, and curves greater than 40° is 0.1 percent.
What do we know about it?
The precise cause of AIS is still largely uncertain. Many theories exist which list genetics, skeletal growth, melatonin deficiency, neuromuscular abnormalities, and metabolic disturbances as possible causes.
- Thoracic curves with the apex on the right are the most common type of curve, followed by a double thoracolumbar curve which is the second most common.
- Only 10% of adolescents with scoliosis have curve progression requiring medical intervention.
- There are three main determinants of scoliotic curve progression: patient gender, curve magnitude at time of diagnosis, and future growth potential.
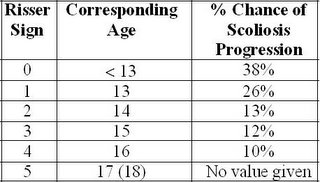
- Curves rarely progress once skeletal maturity is reached. Skeletal maturity can be determined using Risser’s sign.
Risser’s Sign:
Lonstien & Carlson:
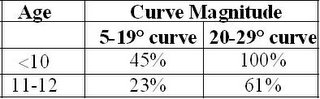
Progression Factor =
How do we manage it?
Curves between 10-15 degrees require no active treatment, but should be monitored every 6 months.
- Curves between 25-40 degrees should be considered for bracing.
- Curves over 30 degrees should be monitored by X-ray every 3 months.
- Curves over 40 degrees should be referred for surgery.
- Alternative to bracing is Lateral Electric Surface Stimulation. This form of treatment has been shown to produce similar results as bracing when measuring curve progression.
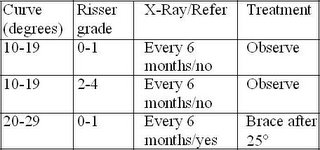
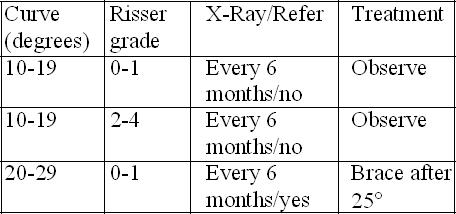
Treatment and Referral Guidelines for Patients with Scoliosis:
Other factors concerning scoliosis:
- The majority of curves spontaneously stabilize themselves and thereby reduce the risk of further curve progression.
- Controversy exists on whether patients with scoliosis have higher incidence of back pain than those without.
- There exists an association between AIS and decreased bone mineral density (osteopenia), however the underlying cause is not known and the curve magnitude does not appear to be linked with the degree of osteopenia.
References:
Cheng, J., Tang S.P., Guo, X. Chan, C., Qin, L. Osteopenia in Adolescent Idiopathic Scoliosis. Spine 2001, E19-E23.
Greiner, K.A. Adolescent Idiopathic Scoliosis: Radiologic Decision-Making. American Family Physician, Vol 65, No. 9, May 15, 2002.
Reamy, B., Joseph Slakey. Adolescent Idiopathic Scoliosis: Review and Current Concepts. American Family Physician, Vol 64, No. 1, July 1 2001.
Disclaimer
This information is not intended to be a substitute for professional medical advice. You should not use this information to diagnose or treat a health problem or disease without consulting with a qualified health care provider. Please consult your health care provider with any questions or concerns you may have regarding your condition. Any attempt to diagnose and treat an illness using the information in this site should come under the direction of a trained medical practitioner. We accept no responsibility for any adverse effects or consequences resulting from the use of any of the suggestions or procedures in this site or related internet links. By using the information in this web site you are confirming that you understand this statement and that you accept all risk and responsibility.
All matters regarding your health should be supervised by your health care provider. All information provided in this site is for the purpose of education, not treatment.
What is it?
Scoliosis is a lateral curvature of the spine (> 10°) in the frontal plane with accompanying rotation of the vertebrae about a longitudinal axis. More specifically, adolescent idiopathic scoliosis (AIS) is a scoliosis of unknown origin that affects children between the ages of approximately 10 and 18 years of age.
Who gets it?
AIS affects approximately 2 percent of children between the ages of 10 and 16. AIS of small curvatures occurs with equal rates in both boys and girls in that age group. However, curves of larger magnitudes (> 30°) occur ten times more often in females then in males. Females also have a greater risk of progression. The prevalence of curves greater than 30° is 0.2 percent, and curves greater than 40° is 0.1 percent.
What do we know about it?
The precise cause of AIS is still largely uncertain. Many theories exist which list genetics, skeletal growth, melatonin deficiency, neuromuscular abnormalities, and metabolic disturbances as possible causes.
- Thoracic curves with the apex on the right are the most common type of curve, followed by a double thoracolumbar curve which is the second most common.
- Only 10% of adolescents with scoliosis have curve progression requiring medical intervention.
- There are three main determinants of scoliotic curve progression: patient gender, curve magnitude at time of diagnosis, and future growth potential.
- Curves rarely progress once skeletal maturity is reached. Skeletal maturity can be determined using Risser’s sign.
Risser’s Sign:

Lonstien & Carlson:
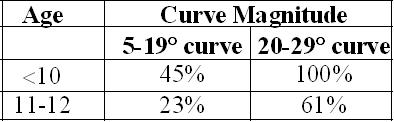
Progression Factor =

How do we manage it?
Curves between 10-15 degrees require no active treatment, but should be monitored every 6 months.
- Curves between 25-40 degrees should be considered for bracing.
- Curves over 30 degrees should be monitored by X-ray every 3 months.
- Curves over 40 degrees should be referred for surgery.
- Alternative to bracing is Lateral Electric Surface Stimulation. This form of treatment has been shown to produce similar results as bracing when measuring curve progression.
Treatment and Referral Guidelines for Patients with Scoliosis:
Other factors concerning scoliosis:
- The majority of curves spontaneously stabilize themselves and thereby reduce the risk of further curve progression.
- Controversy exists on whether patients with scoliosis have higher incidence of back pain than those without.
- There exists an association between AIS and decreased bone mineral density (osteopenia), however the underlying cause is not known and the curve magnitude does not appear to be linked with the degree of osteopenia.
References:
Cheng, J., Tang S.P., Guo, X. Chan, C., Qin, L. Osteopenia in Adolescent Idiopathic Scoliosis. Spine 2001, E19-E23.
Greiner, K.A. Adolescent Idiopathic Scoliosis: Radiologic Decision-Making. American Family Physician, Vol 65, No. 9, May 15, 2002.
Reamy, B., Joseph Slakey. Adolescent Idiopathic Scoliosis: Review and Current Concepts. American Family Physician, Vol 64, No. 1, July 1 2001.
Disclaimer
This information is not intended to be a substitute for professional medical advice. You should not use this information to diagnose or treat a health problem or disease without consulting with a qualified health care provider. Please consult your health care provider with any questions or concerns you may have regarding your condition. Any attempt to diagnose and treat an illness using the information in this site should come under the direction of a trained medical practitioner. We accept no responsibility for any adverse effects or consequences resulting from the use of any of the suggestions or procedures in this site or related internet links. By using the information in this web site you are confirming that you understand this statement and that you accept all risk and responsibility.
All matters regarding your health should be supervised by your health care provider. All information provided in this site is for the purpose of education, not treatment.
posted by Dr. Murray Heber at 9:59 AM
![]()

0 Comments:
Post a Comment
<< Home