Rotator Cuff Injuries and the S.I.C.K. Scapula
Do you suffer from a chronic rotator cuff injury?
The problem may not be the rotator cuff, you might have a S.I.C.K. scapula!
Here's what to look for:
Are you an Overhead Athlete? (Baseball, Volleyball, Tennis…)
Do you have heaviness in your arm with throwing/overhead activities?
Have you ever experienced “Dead Arm”?
Do you suffer from “Shoulder Impingement” or a Rotator Cuff injury?
Have you ever been diagnosed with a SLAP lesion?
If you answered yes to any of these questions, you may have a S.I.C.K. Scapula!
Often diagnosed as a rotator cuff injury, the following will help to illustrate why you may not be getting better with simple rotator cuff treatment and rehabilitation.
The S.I.C.K. scapula is a pneumonic that was developed to help describe a group of findings in the shoulder and scapula (shoulder blade). S.I.C.K. scapula stands for Scapular malposition, Inferior medial scapular winging, Coracoid tenderness, and scapular dysKinesis. First put forward by a group of authors to describe conditions observed in professional baseball players, this new approach to addressing shoulder problems is changing the way shoulder treatment and rehabilitation is viewed. This will all be described in the following article.
First thing to know…Anatomy of the shoulder!
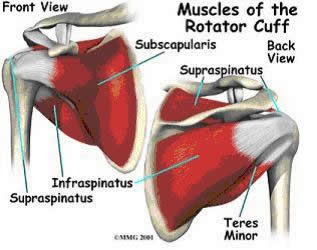
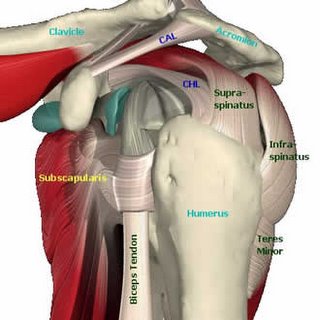
The scapula, commonly called your shoulder blade is the only attachment of your arm to the rest of your body. The scapula is also the origin of very important muscles that move the arm, such as the rotator cuff (Supraspinatous, Infraspinatus, Teres Minor, and Subscapularis muscles) and 9 other muscles that do a variety of work to help you shrug your shoulders, move your arms and even your forearms. The scapula has only one attachment to another bone and that is your clavicle (or collarbone). The clavicle provides the only solid bony attachment of your hand, forearm, and shoulder to the rest of your body!
How can one little bone like your clavicle be responsible for allowing and supporting so much movement in the shoulder, arm, and hand?
The answer is that it has support from a number of muscles that help hold and stabilize your shoulder blade on the back of your rib cage. This becomes very important since without a solid attachment on your body, the shoulder doesn't have a strong base of support to work from and you can get pain/injuries while performing simple tasks like throwing a ball, working overhead or even just doing a push-up.
So how does all this cause the pain you get in your shoulder? According to the work done by Burkhart, Kibler, et al., what they found in professional baseball players with shoulder pain was a greatly decreased range of motion in internal rotation of the throwing shoulder. They linked the decrease in internal rotation with an increase in external rotation and tightening of part of the shoulder capsule. The tightening of the posterior shoulder capsule actually changes the axis of rotation of the shoulder, allowing for the increase in external rotation and decrease in internal rotation. This change in the axis of rotation and resulting increase in external rotation provides an opportunity for the development of a SLAP lesion (Superior Labrum Anterior Posterior). A SLAP lesion is damage to the cartilage (labrum) that helps deepen your shoulder joint. This occurs because the long head of the Biceps Muscle in your arm attaches in this cartilage (labrum) and with more external rotation available in the shoulder, the tendon of the biceps can actually peel this cartilage off of the bone resulting in a SLAP lesion and a significant amount of pain and discomfort.
Another finding in these professional athletes was that they had what is called scapular winging. Scapular winging is when the bottom tip and/or the inside border of the shoulder blade sticks out, or wings away from the rib cage at rest and is exaggerated with certain arm movements. This is often caused by having weak muscles that hold the scapula on the rib cage, most commonly the middle and lower trapezius and the serratus anterior. In addition to weak muscles, there are often tight muscles that help “pull” the scapula off the rib cage. The main muscle that does this is the Pectoralis Minor. This muscle attaches from the ribs on your chest to the coracoid process of the scapula (which is on the top and front of the shoulder just below and deep to the collarbone). When this muscle gets tight, it pulls the scapula up and over the top of the rib cage, resulting in this inferior-medial border winging.
In addition to causing scapular winging, this change in position also causes another change in the axis of rotation of the shoulder joint resulting in early pinching of the humerus against the top of the scapula. This early pinching is most noticeable by raising your arms straight up in front of you. If you get pain in the shoulder, it is sometimes called an impingement syndrome. Now if you push your shoulder blade firmly against your back by leaning on a wall and try raising your arm in front of you, you should get it higher before you feel pain. This is because by pressing your shoulder blade onto your rib cage, you are restoring the proper position of the shoulder blade resulting in a more normal axis of rotation and thereby restoring normal range of motion.
A final finding that was noticed in this group of athletes was that the scapula, which normally moves in a smooth fashion when you raise your arms is now not moving properly. This is called Scapular Dyskinesis. With normal shoulder movement, the inferior tip of the scapula moves outward and upwards. In the SICK scapula, the inferior medial tip does not move in the same fashion as the healthy shoulder and gets “stuck” in a lower position.
As you can see, if you have been doing weeks and months of rotator cuff strengthening exercises with rubber tubing and you still have shoulder pain, you may need to address the muscles that help hold that shoulder blade on your ribcage. Without a strong base of support to work from, the rotator cuff will not be able to fully recover. The shoulder and arm can only get as strong as the muscles that hold the shoulder blade onto your body.
Lets now summarize our S.I.C.K. scapula pneumonic:
S: Scapular malposition on the rib cage
I: Inferior medial border winging from weak middle and lower trapezius muscles
C: Coracoid pain and malposition from the attachment of a tight Pectoralis minor muscle pulling on the coracoid
K: Scapular dyskinesis from alterations in muscle recruitment patterns
Many of the above findings are also present in recreational athletes, office and computer workers. The typical posture of a computer operator is with the head tilted down, shoulders rolled forwards and arms stretched out in front of them. This allows for tightening of the pectoralis minor on the front of the body since the shoulders are already rolled forward. It also allows for the lower trapezius muscle to get weak because of lack of use from not holding your shoulders back. As a result of these tight and weak muscles, the shoulder blades don’t sit properly on the rib cage and when you move your arms, you have alterations in the proper movement patterns. Now you can see how not only professional athletes can suffer from this type of condition. As a result, many people suffer from shoulder pain that is a result of poor shoulder position on the rib cage and from altered muscle firing patterns.
How should this be treated?
The best treatment for the elite professional athlete is physical rehabilitation. The authors found that by stretching the posterior shoulder capsule, strengthening the muscles that hold your scapula in place and stretching/relaxing the tight muscles that pull the scapula into a different position.
Many treatment forms are available for treating this type of condition. Soft tissue techniques such as Active Release Techniques (ART®), Graston, and Medical Acupuncture are designed to address these issues on functional, anatomical, and neurological levels.
Be sure to have a complete physical examination by a qualified healthcare practitioner in order to receive a proper diagnosis and plan of management.
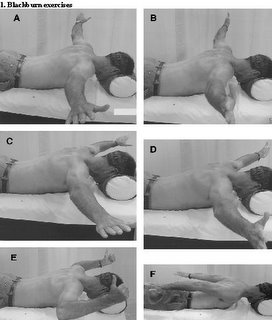
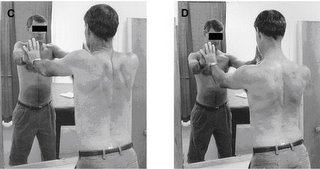
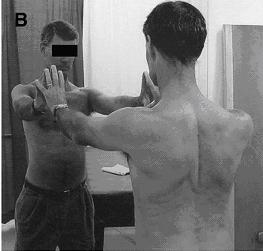
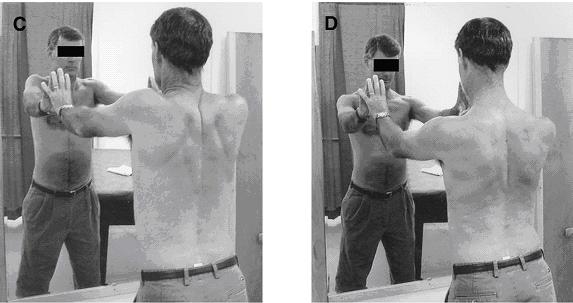
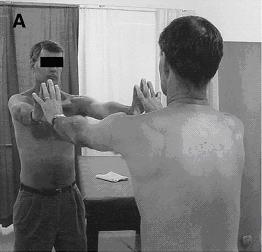
Here is a sample of a few of the rehabilitation exercises that should be performed by someone with a S.I.C.K. scapula as outlined by Burkhart, Morgan and Kibler:
2. Scapular Clock Exercise




References:
Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy. 2003 Apr;19(4):404-20
Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part II: evaluation and treatment of SLAP lesions in throwers.Arthroscopy. 2003 May-Jun;19(5):531-9
Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation.Arthroscopy. 2003 Jul-Aug;19(6):641-61
Kibler WB, Uhl TL, Maddux JW, Brooks PV, Zeller B, McMullen J. Qualitative clinical evaluation of scapular dysfunction: a reliability study. J Shoulder Elbow Surg. 2002 Nov-Dec;11(6):550-6.
Rubin BD, Kibler WB. Fundamental principles of shoulder rehabilitation: conservative to postoperative management. Arthroscopy. 2002 Nov-Dec;18(9 Suppl 2):29-39.
Kibler WB, McMullen J. Shoulder rehabilitation strategies, guidelines, and practice. Orthop Clin North Am. 2001 Jul;32(3):527-38
Kibler WB, Livingston B. Closed-chain rehabilitation for upper and lower extremities. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):412-21
Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg. 2003 Mar-Apr;11(2):142-51
Disclaimer
This information is not intended to be a substitute for professional medical advice. You should not use this information to diagnose or treat a health problem or disease without consulting with a qualified health care provider. Please consult your health care provider with any questions or concerns you may have regarding your condition. Any attempt to diagnose and treat an illness using the information in this site should come under the direction of a trained medical practitioner. We accept no responsibility for any adverse effects or consequences resulting from the use of any of the suggestions or procedures in this site or related internet links. By using the information in this web site you are confirming that you understand this statement and that you accept all risk and responsibility.
All matters regarding your health should be supervised by your health care provider. All information provided in this site is for the purpose of education, not treatment.
Do you suffer from a chronic rotator cuff injury?
The problem may not be the rotator cuff, you might have a S.I.C.K. scapula!
Here's what to look for:
Are you an Overhead Athlete? (Baseball, Volleyball, Tennis…)
Do you have heaviness in your arm with throwing/overhead activities?
Have you ever experienced “Dead Arm”?
Do you suffer from “Shoulder Impingement” or a Rotator Cuff injury?
Have you ever been diagnosed with a SLAP lesion?
If you answered yes to any of these questions, you may have a S.I.C.K. Scapula!
Often diagnosed as a rotator cuff injury, the following will help to illustrate why you may not be getting better with simple rotator cuff treatment and rehabilitation.
The S.I.C.K. scapula is a pneumonic that was developed to help describe a group of findings in the shoulder and scapula (shoulder blade). S.I.C.K. scapula stands for Scapular malposition, Inferior medial scapular winging, Coracoid tenderness, and scapular dysKinesis. First put forward by a group of authors to describe conditions observed in professional baseball players, this new approach to addressing shoulder problems is changing the way shoulder treatment and rehabilitation is viewed. This will all be described in the following article.
First thing to know…Anatomy of the shoulder!

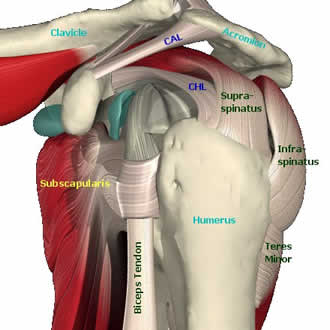
The scapula, commonly called your shoulder blade is the only attachment of your arm to the rest of your body. The scapula is also the origin of very important muscles that move the arm, such as the rotator cuff (Supraspinatous, Infraspinatus, Teres Minor, and Subscapularis muscles) and 9 other muscles that do a variety of work to help you shrug your shoulders, move your arms and even your forearms. The scapula has only one attachment to another bone and that is your clavicle (or collarbone). The clavicle provides the only solid bony attachment of your hand, forearm, and shoulder to the rest of your body!
How can one little bone like your clavicle be responsible for allowing and supporting so much movement in the shoulder, arm, and hand?
The answer is that it has support from a number of muscles that help hold and stabilize your shoulder blade on the back of your rib cage. This becomes very important since without a solid attachment on your body, the shoulder doesn't have a strong base of support to work from and you can get pain/injuries while performing simple tasks like throwing a ball, working overhead or even just doing a push-up.
So how does all this cause the pain you get in your shoulder? According to the work done by Burkhart, Kibler, et al., what they found in professional baseball players with shoulder pain was a greatly decreased range of motion in internal rotation of the throwing shoulder. They linked the decrease in internal rotation with an increase in external rotation and tightening of part of the shoulder capsule. The tightening of the posterior shoulder capsule actually changes the axis of rotation of the shoulder, allowing for the increase in external rotation and decrease in internal rotation. This change in the axis of rotation and resulting increase in external rotation provides an opportunity for the development of a SLAP lesion (Superior Labrum Anterior Posterior). A SLAP lesion is damage to the cartilage (labrum) that helps deepen your shoulder joint. This occurs because the long head of the Biceps Muscle in your arm attaches in this cartilage (labrum) and with more external rotation available in the shoulder, the tendon of the biceps can actually peel this cartilage off of the bone resulting in a SLAP lesion and a significant amount of pain and discomfort.
Another finding in these professional athletes was that they had what is called scapular winging. Scapular winging is when the bottom tip and/or the inside border of the shoulder blade sticks out, or wings away from the rib cage at rest and is exaggerated with certain arm movements. This is often caused by having weak muscles that hold the scapula on the rib cage, most commonly the middle and lower trapezius and the serratus anterior. In addition to weak muscles, there are often tight muscles that help “pull” the scapula off the rib cage. The main muscle that does this is the Pectoralis Minor. This muscle attaches from the ribs on your chest to the coracoid process of the scapula (which is on the top and front of the shoulder just below and deep to the collarbone). When this muscle gets tight, it pulls the scapula up and over the top of the rib cage, resulting in this inferior-medial border winging.
In addition to causing scapular winging, this change in position also causes another change in the axis of rotation of the shoulder joint resulting in early pinching of the humerus against the top of the scapula. This early pinching is most noticeable by raising your arms straight up in front of you. If you get pain in the shoulder, it is sometimes called an impingement syndrome. Now if you push your shoulder blade firmly against your back by leaning on a wall and try raising your arm in front of you, you should get it higher before you feel pain. This is because by pressing your shoulder blade onto your rib cage, you are restoring the proper position of the shoulder blade resulting in a more normal axis of rotation and thereby restoring normal range of motion.
A final finding that was noticed in this group of athletes was that the scapula, which normally moves in a smooth fashion when you raise your arms is now not moving properly. This is called Scapular Dyskinesis. With normal shoulder movement, the inferior tip of the scapula moves outward and upwards. In the SICK scapula, the inferior medial tip does not move in the same fashion as the healthy shoulder and gets “stuck” in a lower position.
As you can see, if you have been doing weeks and months of rotator cuff strengthening exercises with rubber tubing and you still have shoulder pain, you may need to address the muscles that help hold that shoulder blade on your ribcage. Without a strong base of support to work from, the rotator cuff will not be able to fully recover. The shoulder and arm can only get as strong as the muscles that hold the shoulder blade onto your body.
Lets now summarize our S.I.C.K. scapula pneumonic:
S: Scapular malposition on the rib cage
I: Inferior medial border winging from weak middle and lower trapezius muscles
C: Coracoid pain and malposition from the attachment of a tight Pectoralis minor muscle pulling on the coracoid
K: Scapular dyskinesis from alterations in muscle recruitment patterns
Many of the above findings are also present in recreational athletes, office and computer workers. The typical posture of a computer operator is with the head tilted down, shoulders rolled forwards and arms stretched out in front of them. This allows for tightening of the pectoralis minor on the front of the body since the shoulders are already rolled forward. It also allows for the lower trapezius muscle to get weak because of lack of use from not holding your shoulders back. As a result of these tight and weak muscles, the shoulder blades don’t sit properly on the rib cage and when you move your arms, you have alterations in the proper movement patterns. Now you can see how not only professional athletes can suffer from this type of condition. As a result, many people suffer from shoulder pain that is a result of poor shoulder position on the rib cage and from altered muscle firing patterns.
How should this be treated?
The best treatment for the elite professional athlete is physical rehabilitation. The authors found that by stretching the posterior shoulder capsule, strengthening the muscles that hold your scapula in place and stretching/relaxing the tight muscles that pull the scapula into a different position.
Many treatment forms are available for treating this type of condition. Soft tissue techniques such as Active Release Techniques (ART®), Graston, and Medical Acupuncture are designed to address these issues on functional, anatomical, and neurological levels.
Be sure to have a complete physical examination by a qualified healthcare practitioner in order to receive a proper diagnosis and plan of management.
Here is a sample of a few of the rehabilitation exercises that should be performed by someone with a S.I.C.K. scapula as outlined by Burkhart, Morgan and Kibler:

2. Scapular Clock Exercise



References:
Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy. 2003 Apr;19(4):404-20
Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part II: evaluation and treatment of SLAP lesions in throwers.Arthroscopy. 2003 May-Jun;19(5):531-9
Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation.Arthroscopy. 2003 Jul-Aug;19(6):641-61
Kibler WB, Uhl TL, Maddux JW, Brooks PV, Zeller B, McMullen J. Qualitative clinical evaluation of scapular dysfunction: a reliability study. J Shoulder Elbow Surg. 2002 Nov-Dec;11(6):550-6.
Rubin BD, Kibler WB. Fundamental principles of shoulder rehabilitation: conservative to postoperative management. Arthroscopy. 2002 Nov-Dec;18(9 Suppl 2):29-39.
Kibler WB, McMullen J. Shoulder rehabilitation strategies, guidelines, and practice. Orthop Clin North Am. 2001 Jul;32(3):527-38
Kibler WB, Livingston B. Closed-chain rehabilitation for upper and lower extremities. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):412-21
Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg. 2003 Mar-Apr;11(2):142-51
Disclaimer
This information is not intended to be a substitute for professional medical advice. You should not use this information to diagnose or treat a health problem or disease without consulting with a qualified health care provider. Please consult your health care provider with any questions or concerns you may have regarding your condition. Any attempt to diagnose and treat an illness using the information in this site should come under the direction of a trained medical practitioner. We accept no responsibility for any adverse effects or consequences resulting from the use of any of the suggestions or procedures in this site or related internet links. By using the information in this web site you are confirming that you understand this statement and that you accept all risk and responsibility.
All matters regarding your health should be supervised by your health care provider. All information provided in this site is for the purpose of education, not treatment.
posted by Dr. Murray Heber at 11:02 AM
![]()

{kind=link}
12 Comments:
Very nice Info. I am preparing for MSc Assignment in SportsMEdicine in UK. CAn I use your article and is it published somewhere. If it is can you please send me a link?
Also can I use the refrences . Are hey in a word prcessor. It would save me tying thee refeerences alltogether.
This is a very informative post. Your description of the condition is excellent as is your prescription for recovery.
Chris - the Rotater
This article definately needs a lot more love. I was diagnosed with a case of the S.I.C.K. scapula today - its the only thing that has fit in with me getting coracoid pain/tenderness when doing internal rotations (from which i understand is due to improper movement/joint position).
curiously I notice that my shoulder joint tends to stick out when doing say dips, while my right shoulder makes a small but noticeable movement backwards with my rhomboids/middle traps.
would you say this is due to having an inactive subscap/lower traps/rhomboids?
Thanks for the article!
can i have your personnel email or contact no???? please i extremely need your help
hope for a positive reply
faisal_heaven2000@yahoo.com
preferred one
yo tengo este sindrome pero ademas tengo inestabilidad por hiperlaxitud todo esto puede ser consecuencia o depender uno de lo otro, la solucion es una artroscopia y un plan de reforzamiento muscular, ustedes q opinan,seria bueno una opinion de su parte mi correo es yulianarcila@hotmail.com
I was diagnosed today, im 18 and had no idea pitching for so long as a child and middle school caused my pain. I actually quit playing because the pain was debilitating. Now im informed and happy to recieve treatment. Thx lensgraph
I was diagnosed today, im 18 and had no idea pitching for so long as a child and middle school caused my pain. I actually quit playing because the pain was debilitating. Now im informed and happy to recieve treatment. Thx lensgraph
I was diagnosed today, im 18 and had no idea pitching for so long as a child and middle school caused my pain. I actually quit playing because the pain was debilitating. Now im informed and happy to recieve treatment. Thx lensgraph
Thanks for the informative post, will be linking back on my blog!
I like the article, but am not a big fan of the exercises that are given to "rehab" the shoulder.
As a shoulder specialist, most of my clients that have this pathology can not even get into the positions that are shown. To be honest, I would advise them not to. It is a position of instability of the joint. If you have pain while trying to do those exercises, you are having mechanical failure of the joint, and irritating already weak tissues. The last thing you want in your glenohumeral joint is inflammation.
If you are going to strengthen the muscles, do it in a position that the joint is not stressed further.
The scapular clock is great, and to that I would add a seated row, and external rotation. That is all most shoulders need.
I agree that it's important to think carefully about what the underlying reason is for a website, the dogs example fits the bill perfectly :)
auto injury doctor
Post a Comment
<< Home