Cyclist’s palsy, or sometimes called Handlebar palsy is a relatively common condition for road cyclists and mountain bikers. This palsy is a nerve injury at the wrist and until recently, has not been receiving much attention in the literature. First reported in European literature in 1896 by Destot, the condition got very little attention until it appeared in North American literature in 1975 by Eckman et al. Even then, the only published research were case reports which dealt strictly with findings in individual cases and no research was done to examine the exact mechanism or location of the nerve injury. More recent research has been designed to look closely at the Ulnar and even Median nerves at the wrist and look at the effect of cycling on nerve conduction. Below is a summary of the research done to this point in time.
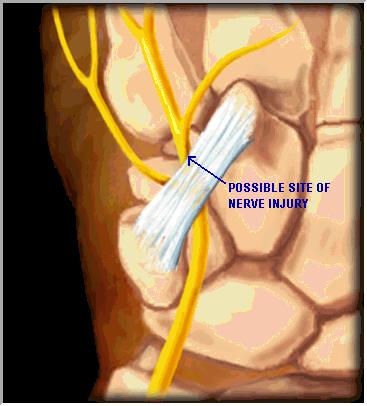
The Ulnar nerve is a branch of the brachial plexus that provides sensation and motor supply to the upper extremity. The Ulnar nerve specifically is responsible for providing sensation and motor innervation to the medial (or inside) of the forearm and hand. The brachial plexus comes out at the neck, between muscles known as the scalenes, and then traverses the length of the arm before crossing the elbow after which it divides into its respective terminal branches. After passing the elbow, the ulnar nerve divides and gives off 2 sensory branches which supply sensation to parts of the back of the hand and the little finger and half of the ring finger. At the wrist, the ulnar nerve enters the hand by passing through Guyon’s Canal. This is a tight tunnel that is formed between 2 of the bones in your wrist (the pisiform and hamate bones) and the ligaments that join these bones together (pisohamate ligament). Either within or just beyond the canal, the ulnar nerve divides again in to two motor branches which supply some of the muscle in the hand and fingers. These branches are the branch to the hypothenar and the deep motor branch of the ulnar nerve. These innervate the muscles that help move the little finger and thumb respectively.

It is within Guyon’s Canal that the ulnar nerve is thought to get injured with cycling and depending on the exact point of injury, symptoms may vary from person to person. Since the sensory branches of the ulnar nerve are given off before or early into the canal, sensory loss is not found in all cases and is in fact a rare finding in cyclist’s palsy. The most common finding is that of weakness and clumsiness of the hand and thumb. Often people who develop this condition complain of numbness or tingling in the hand that goes away within a day or two but then they have persistent weakness with pinching and fine finger movements such as playing the piano.
The reason for the above symptoms is simple. While cycling, the position of the hands while holding the handlebars places pressure on the ulnar nerve in the canal. With either multi-day road cycling events or a single day of mountain biking, that pressure combined with vibrations from the road or trails is enough to damage the nerve and causes what is called a neuropraxia. A neuropraxia is a focal injury to a nerve that does not allow for conduction of a nerve impulse past the site of injury. The nerve functions normally both proximal and distal to the site of injury, and it is because of demyelination (loss of the protective nerve coating) at the site of injury that the nerve stops working and the muscles beyond that point get weak.
Ulnar Nerve at the Wrist
The good news about this type of nerve injury is that it is self–limiting, meaning that the nerve will regenerate on its own and function of the muscles will be restored. In a review by Capitani and Beer (2002), they found that within 3 months of the onset of symptoms and stopping the mechanism of injury, all motor function in the hand was restored to normal. It is important to know about this condition so that you can take steps to avoid it. A study by Akuthota et al found that long-distance bicycling caused a slowing of nerve impulses along the deep branch of the ulnar nerve in all of the cyclists in the study. They didn’t necessarily damage the nerve to the point of neuropraxia, but they did damage it enough to slow the conduction velocity. This shows how all long-distance cyclists are at risk of developing this condition. This same study also showed an exacerbation of Median nerve symptoms in a cyclist with carpal tunnel syndrome. This was due to wrist position on the handlebars. If your hands are on the handlebars in such a way that the wrist is held in extension, this can exacerbate carpal tunnel symptoms.
Tips to avoid placing too much stress on the hands and the Median and Ulnar nerves are:
- Wear padded gloves and/or ride with padded handlebars to minimize the vibration forces on your wrist and hands.
- Avoid direct pressure over the area of Guyon’s canal by avoiding resting the medial aspect of your wrist on the handlebars.
- Avoid letting your wrists rest in excessive extension.
- Make sure you have a proper seat height and sitting position. This will help minimize the amount of weight you place on your wrists.
- Select a proper choice of handlebar. The type of handlebar can also affect the amount of pressure you place through your wrists.
- More specifically for mountain biking, it is important to have good shocks on the front forks of your bike. They help to absorb and dampen the repetitive vibrations and impact on your wrist while on rough terrain.
To summarize, research has shown that long-distance bicycling slows the conduction time in the deep motor branch of the ulnar nerve which supplies the muscle in the thumb used for pinching and grasping. Research has also shown pre-existing nerve palsies, such as carpal tunnel syndrome, can be aggravated with long distance cycling. Furthermore, it has been found that cyclist’s palsy can be brought on by a single day of mountain biking. It is important to know the signs and symptoms of this condition so that it can be easily identified and a proper diagnosis established without having to go for numerous tests and possible surgery which can lead to lost days of work and loss of income. It is also very important to find a healthcare professional who can identify this condition and who knows how it is best treated. As previously mentioned, Capitani et al found that within three months, all or near all of the lost motor function was restored. Interestingly, Padua et al published a case of cyclist’s palsy that was treated by surgically releasing the ulnar nerve in Guyon’s canal. The patient was sent for surgery after the symptoms persisted for one month. It was reported that three months after surgery the patient recovered most of the motor function to the hand. Knowing the natural history of the cyclist’s palsy, one may be able to avoid unnecessary surgical intervention that will only serve to lengthen the recovery period. An accurate diagnosis is typically made by having a history of cycling, hand muscle weakness or clumsiness with no sensory loss. The diagnosis is confirmed with nerve conduction studies that show a decrease or loss of nerve conduction past guyon’s canal.
Key Concepts to Remember:
References:
Akuthota V, Plastaras C, Lindberg K, Tobey J, Press J, Garvan C. The Effect of Long-Distance Bicycling on Ulnar and Median Nerves: An Electrophysiologic Evaluation of Cyclist Palsy. American Journal of Sports Medicine. 33 (8), 2005, pp 1224-1230.
Padua L, Insola A, LoMonaco M, Denaro FG, Padua R, Tonali P. A Case of Guyon Syndrome with Neuropraxic Block Resolved after Surgical Decompression. Electroendephalography and Clinical Neurophysiology. 109, 1998, pp. 191-193.
Capitani D, Beer S. Handlebar Palsy – acompression syndrome of the deep terminal (motor) branch of the ulnar nerve in biking. J Neurology. 249, 2002. pp. 1441-1445.
McIntosh KA, Preston DC, Logigian EL. Short-segment incremental studies to localize ulnar nerve entrapment at the wrist. American Academy of Neurology. 50 (1), 1998. pp. 303-306.
posted by Dr. Murray Heber at 11:02 AM
7 comments
![]()
